A diagnosis of cancer can feel overwhelming. We are here to help with information to support the next steps of your journey, and we hope these resources help you approach your breast cancer decision-making with more clarity. When preparing for surgery, understanding the tools and terms available can help you feel more confident as you talk with your medical team about your choices.
What Are Surgical Margins and why do they matter during a lumpectomy?
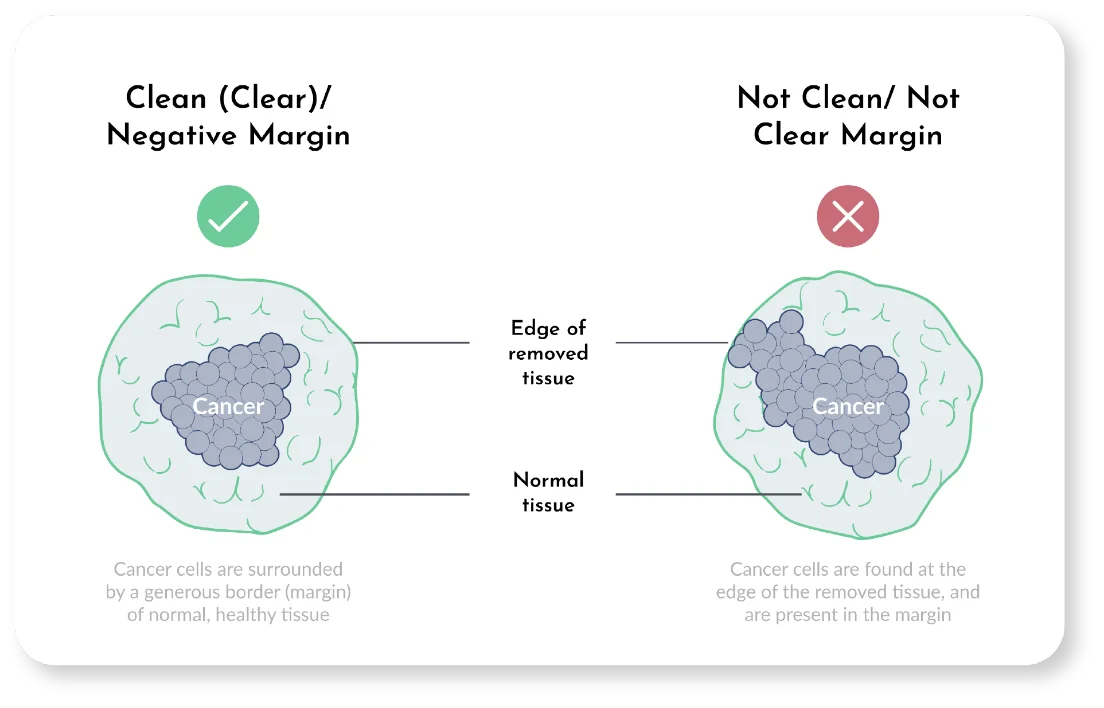
Your surgeon will remove the cancerous tumor and some normal tissue—the margin—that surrounds it. After the procedure, a pathologist will carefully examine the tissue to see if cancer cells are present in the margins. This report typically takes 2-7 days to get back.
Margins that are free of cancer are called “negative” or “clean.” Margins that have cancer cells in them are called “positive.” and not considered clean 10
Ideally, surgeons will know if the margins are negative (no cancer) during the procedure. If not, they can remove more tissue if needed until margins are clean.
In some cases, an additional surgery, called a re-excision, may be needed after your first lumpectomy. If the pathology from your lumpectomy reveals that the margins are close or not clear, your surgeon may recommend a second surgery to help achieve clear margins. This could be another lumpectomy (re-excision) or, in certain cases, a mastectomy.
Advanced Clarity in the OR
Advanced imaging technologies, like Perimeter’s Claire, provide microscopic clarity while you are still in the operating room. This “extra set of eyes” is designed to help your surgeon evaluate the removed tissue in real-time. By providing more information during the initial procedure, these tools support your surgical team’s goal of identifying areas that may need further attention before the surgery is complete.
Choosing Between a Lumpectomy and a Mastectomy
In some cases, you may be offered the choice of which surgery you would prefer. If your surgical team has offered you a choice between a lumpectomy and a mastectomy, it means that both options are effective for your breast cancer diagnosis.
In some cases, you may be offered the choice of which surgery you would prefer. If your surgical team has offered you a choice between a lumpectomy and a mastectomy, it means that both options are effective for your breast cancer diagnosis.

LUMPECTOMY
The goal of a lumpectomy is to remove the cancer while preserving as much of your breast as possible. Your surgeon will remove the cancer along with a rim of healthy tissue (the margin).

MASTECTOMY
This surgery removes all of the breast tissue in one or both of your breasts. If you have a mastectomy, you can also choose whether you would like to have reconstruction or prefer to stay flat after surgery.
Meet some of the surgeons across the U.S. using Perimeter’s FDA-cleared S-Series OCT technology for margin visualization in the OR.
This is an opportunity for a shared decision-making process—a series of conversations between you and your surgical team to help you make a choice that aligns with your personal values and preferences.

Click the ![]() symbol below to view the answer for any question.
symbol below to view the answer for any question.
Margins refer to the rim of tissue around a cancerous tumor that is removed. The goal is to get “clean” or “negative” margins, meaning there are no remaining cancer cells around the edges of the tumor that could be left in the body with the potential to spread.
While surgeons are continuously working to lower the percentage of repeat surgeries (also called re-excisions or re-operations), studies show it is not uncommon—approximately 1 in 5 for some types of cancer. In breast cancer surgery, 23% of lumpectomies4 require another surgery to get clean margins, while positive surgical margins are found in 11.5% of thyroid cancers and 21% of prostate cancers.
Yes, the Perimeter S-Series OCT imaging device was FDA cleared in February 2021 and became commercially available in the United States that year.
Yes, the Perimeter Claire OCT system was FDA approved in March 2026 and became commercially available in the United States that year.
Perimeter’s device uses high-definition Optical Coherence Tomography (OCT) imaging to visualize margins at the cellular level in the operating room. Images have 10X higher resolution than ultrasound and X-ray and 100X higher than MRI, down to 2mm depth. This gives surgeons the clarity they need during the surgery, as they work to achieve clean margins in an effort to avoid another procedure.
Rather than a one-size-fits-all approach that could potentially remove more tissue than is needed, this technology allows surgeons to visualize your margins and tailor your care.
Yes. Optical Coherence Tomography (OCT), developed out of Massachusetts Institute of Technology (MIT) in 1991, has been successfully used in ophthalmology, cardiology and dermatology for decades. The Perimeter S-Series OCT is the first device to use OCT for margin visualization in the operating room.
Yes. Your surgeon will remove the tumor, and it will be taken to the device for scanning. There is no radiation, and the device does not touch the patient or enter the sterile area in the operating room.
Each scan takes 1-2 minutes or about 15 minutes overall, depending on your specific case. The scans are incorporated into the routine workflow of your operation, with limited impact on overall surgery time.
No. OCT adds to your surgeon’s confidence level in real time during surgery, prior to the Pathology report, which is typically final 2-7 days after your surgery.
Pathology remains the “gold standard” as a final assessment of margin status to confirm whether or not cancer remains in the margins.